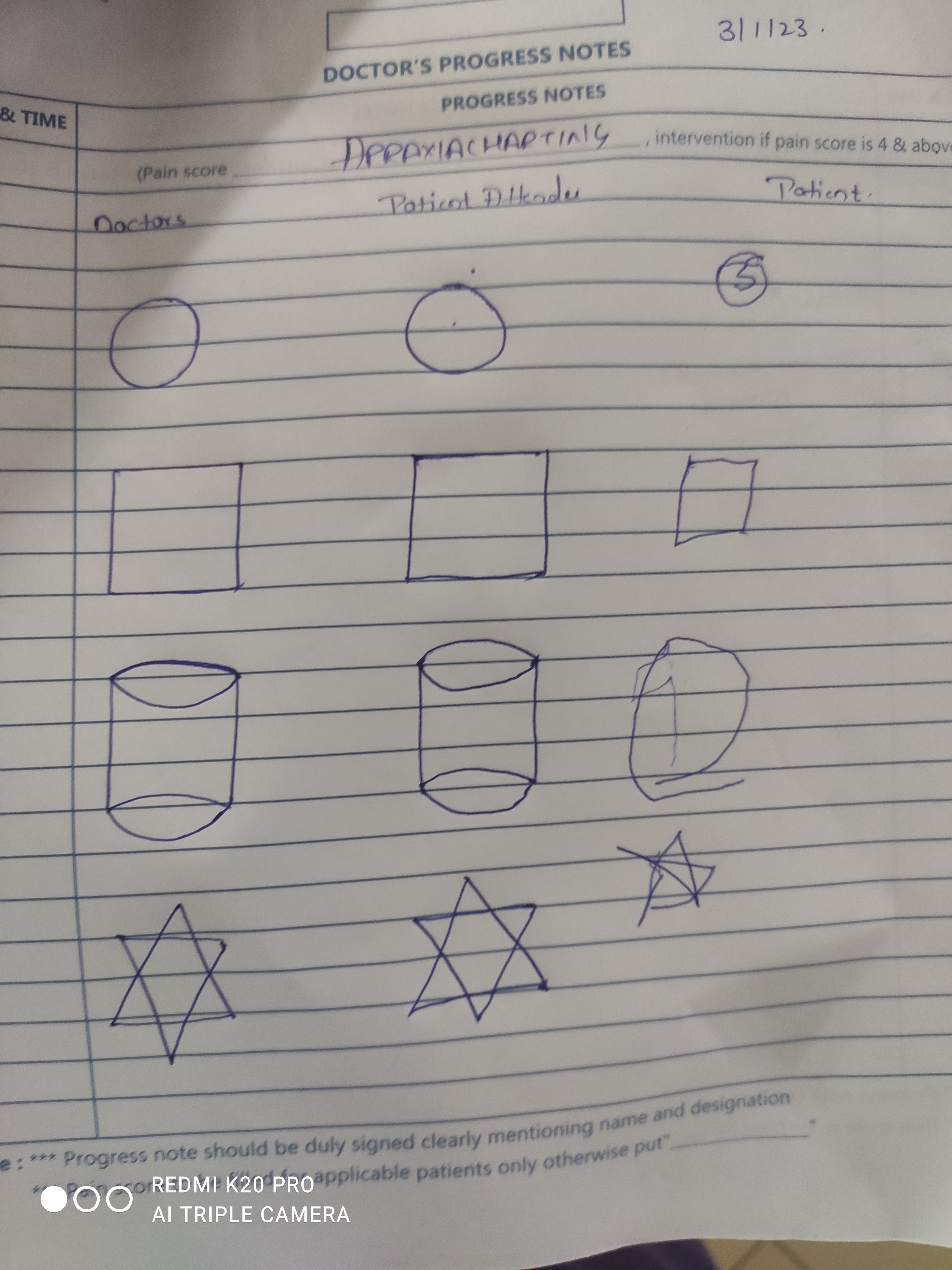
50 F altered sensorium secondary to ?dengue encephalitis? Hepatic encephalopathy ? Uremic encephalopathy? Which form a part of expanded dengue syndrome.
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan
50yr old female came to casualty with complaints of fever since 7days
C/o dry cough since 7days
C/o breathlessness since 4days
C/o abdominal distension since 4days
C/o decreased urine output since 4days
History of present illness
she was apparently alright 7days ago then she developed fever associated with chills insidious in onset, not associated with myalgia or arthralgia
H/o dry cough since 7days , no seasonal variation or diurnal variation , not associated with blood, fever associated with decrease in appetite
On day 1 of illness she sought for consultation at RMP, and was taking treatment at home
On day 3 of illness, she was having c/o breathlessness gradually progressive from grade 1 to 5 HYHA
H/o abdominal distension since 4days gradually progressive to present size associated with abdominal pain
No sob or no c/o PND / Orthopnea
H/o decreased urinary output since 4days
No hematuria, blood in stools or other bleeding manifestations complaints
C/o giddiness since 4days
No c/o hematuria/ear ache /vertigo
K/c/o type 2DM since 1 year
Surger referral notes:

Nephrology referral notes:


Personal history :
Appetite: decreased
Diet: mixed
Bowel and bladder: regular
Sleep: adequate
Addictions: occasional alcoholic and toddy drinker
Menstrual history:
Age of menarch: 12 years
Cycles regular
Attained menopause
Obstretric history: nulliparous
Family history: insignificant
General examination :
Patient was conscious coherent and cooperative at the time of admission
Pallor: present

Icterus: present

Cyanosis
Clubbing
Lymphadenopathy
Edema
Local examination
Petechiae seen on arm and fore arm






Vitals:
GCS: E2V5M3 improved to E4V5M4 on31/12/22
E4V5M6 on1/1/23
Temp:

Vitals:
GCS: E2V5M3 improved to E4V5M4 on31/12/22
E4V5M6 on1/1/23
Temp:



Bp: 130/80 mmHg
HR: 82 bpm
Spo2: 98%on ra
Grbs:




Apraxia chart:


8pm: 415 mg/dl insulin@ 6ml/hr(31/12/22)
10pm:573 mg/dlinsulin@8ml/hr
2am: 339mg/dl@4ml/hr
7am:276mg/dl@3ml/hr
9am:312mg/dl@3ml/hr
I/O: 2750/900ml
5/1/23
8am: 312 mg/dl (1/1/23)
1pm:246 mg/dl 8u Hai given
3pm:232mg/dl
5pm:180mg/dl
7pm: 179 mg)dl
9pm:212mg/dl :8uHai given
12am: 297mg/dl
6am:214mg/dl 4u hai given
I/O: 1900/1050ml
Systemic examination:
CNS:
Level of consciousness: conscious and slightly irritable
Patient was conscious coherent cooperative on1/1/23
Speech; not able to speak
Normal on1/1/23
Nomeningeal signs
Cranial nerves ;
1) olfactory nerve ; percieves smell on both sides
2) optic nerve : normal visual acuity
3) occlomotor nerve ; normal
4) trochlear nerve ; normal
6) abducens nerve ; normal
(3,4,6 cranial nerves) ; ptosis,squint, nystagmus - absent.
* Ocular movements- present in upward,downward,temporal,nasal gaze
* Pupil- size- normal,shape- central
* Visual reflexes- direct, indirect- reacting to light
5) Trigeminal nerve ; cutaneous sensibility over skin and mucous membranes - present
✓ corneal reflex- present on both sides
✓ deviation of jaw on opening mouth- absent
7) facial nerve; normal
8) vestibuli cochlear nerve; normal
9) glossopharyngeal nerve; Taste sensation on posterior 1/3rd of tongue - present on both sides
✓palatal reflex- present on both sides
10)vagus nerve ; no history of regurgitation of fluids through nose
Palatal reflex- present
11) spinal accessory nerve ; normal
12) hypoglossal nerve ; normal
Motor system
Gait: not able to walk
Power U/L L/L
Right 2/5 restrained
Left 2/5 restrained
Tone U/L L/L
Right Normal Normal
Left Normal Normal
Reflexes Biceps triceps supinator knee ankle
Right + + - +. -
Left + +. - +. -
On1/1/23
Tone: normal in all limbs
Power: U/L. L/L
RT. 4/5 3/5
LT. 4/5 3/5
Reflexes: B T S K A. P
RT. : +. + + +. -. Flexion
LT. : + + + +. - flexion
Cerebellar signs : no
No meningeal signs
2/1/23
GCS: E4V5M6
Tone: normal in all limbs
Power: U/L. L/L
RT. 4/5 4/5
LT. 5/5 5/5
Reflexes: B T S K A. P
RT. : ++ + - +. -. Flexion
LT. : + + - +. - flexion
Cerebellar signs : no
No meningeal signs
3/1/23:
GCS: E4V5M6
Tone: normal in all limbs
Power: U/L. L/L
RT. 4/5 4/5
LT. 4/5 4/5
Reflexes: B T S K A. P
RT. : ++ ++ + ++ + Flexion
LT. : ++ + + ++ + flexion
Cerebellar signs : no
No meningeal signs
Pupil : reacting to light
Conjunctival reflex +
Corneal reflex+
Sensory system ; normal
No cerebellar signs
No meningeal signs
CVS:
RS:
Per abdomen:


Provisional diagnosis:
1. Dengue hemorrhagic fever or expanded dengue fever with polyserositis ( resolved)
2. Altered sensorium (resolved) secondary to?dengue encephalitis/hepatic/ uremic encephalopathy
3. With prerenal acute kidney injury
4. Acute liver injury
6.Grade-1 bed sores
5. Known case of type 2 DM
Investigations:
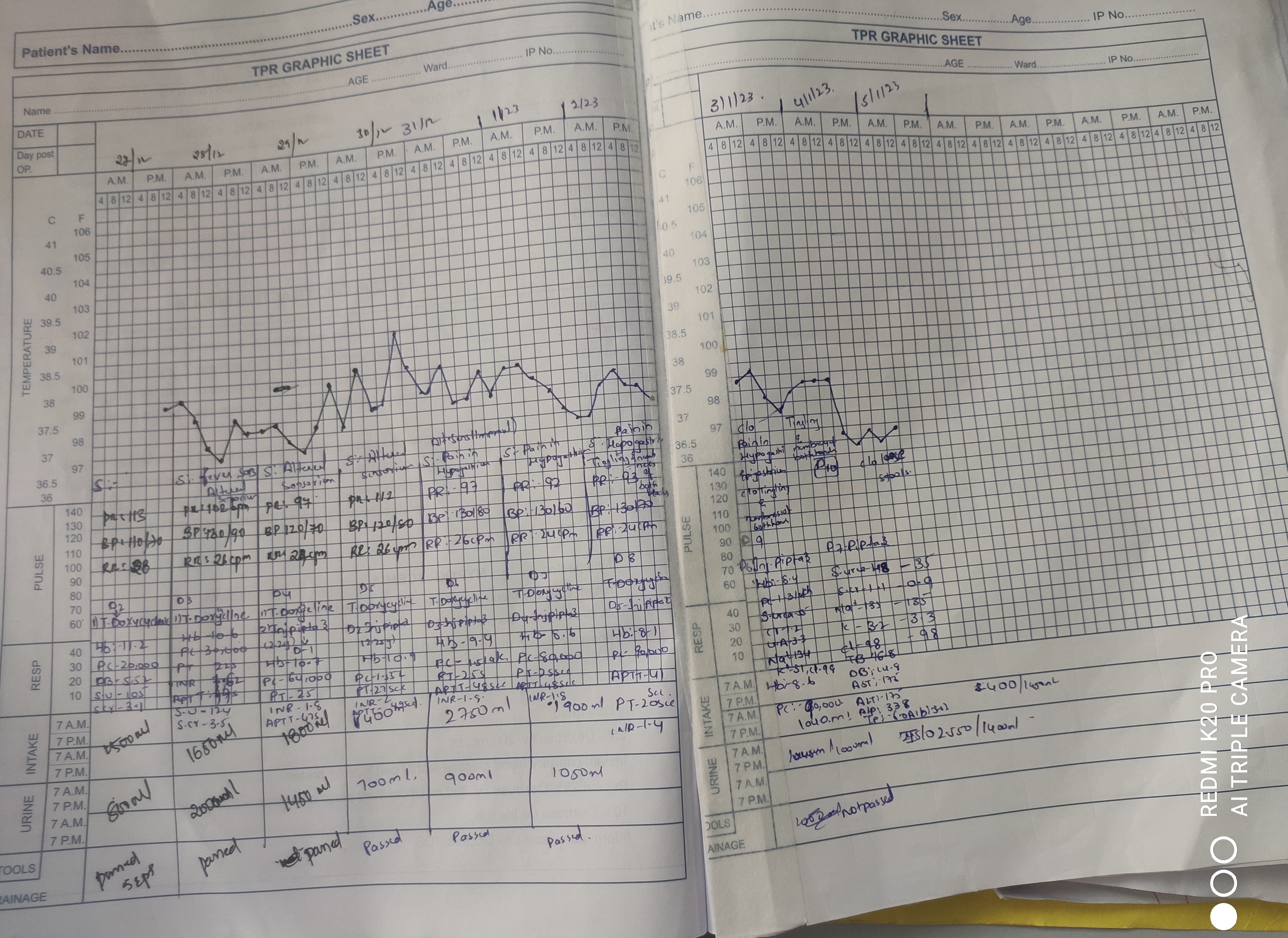
Hemogram
Day-1. Day -2. Day-3. Day-4. Day-5
HB: 11.2g/dl. - 10.6 g/dl. 10.7 g/dl. 10.9. 9.4
D-6:8.6 Day 7: 8.2 d-8: 8.4 d-9:9.6
Plt c: 20,000. 30,000. 64,000. 1.55 lakh. 1.5 lakh d-6: 80,000 Day7:90,000 d-8: 1.3 lakhs d-9: 90,000
TLC:13.300. -. 12,600 12,500. 15,300. 16,000 d-6: 13,200 day7: 13,000 d-8: 9,200 d-9:8200
Lymphocytes: 30. 30. 30. . 14. 08
Monocytes:10. 10. 13. 10. 19
Neutrophils:60. 60. 60. 75. 82
Eosinophils:00. 00. 01 01. 00
Impression : Normocytic normochromic anemiawith leukocytosis and thrombocytopenia
Day-3 microcytic hypochromic Anemia with leukocytosis and thrombocytopenia
Day-4: Normocytic normochromic blood picture with leukocytosis
Day-5: Normocytic normochromic Anemia with neutrophilic leukocytosis
Day-6: Normocytic normochromic Anemia with neutrophilic leukocytosis and thrombocytopenia
Day7: Normocytic normochromic Anemia with thrombocytopenia
Blood group and typing: o positive
28/12/22 Day-1 Day-2. Day-3. Day-4
PT:. 22secs. 25secs. 27 secs
INR:. 1.62. 1.8. 2
Aptt:. 44secs 47 secs. 49secs
Day-5:
PT: 25 secs,Aptt: 48secs. , INR: 1.8
D6-pT: 20 secs,Aptt:44sec,INR: 1.4
D7-PT: 29secs,Aptt:41secs,INR:1.4
Reticulocyte count
Esr: 30
CUE:
Appearance: clear
Albumin: +
Sugars: nil
Pus cells: 3-6
Epithelial cells: 2-4
Rbcs: nil
Urine for ketone bodies: negative
31/12/22:
Appearance: clear
Albumin: +
Sugars: nil
Pus cells: loaded
Epithelial cells: 4-5
Rbcs: 4-5
Epithelial casts:4-5
Others: candida budding yeast hyphae
RBS: 76
FBS: 199
Plbs:
Hba1c: 7.5%
Thyroid profile:
T3: 0.58
T4: 7.60
TSH:0.40
Serology: negative
LFT: d -1 D-2. D-3 D-4. D-5
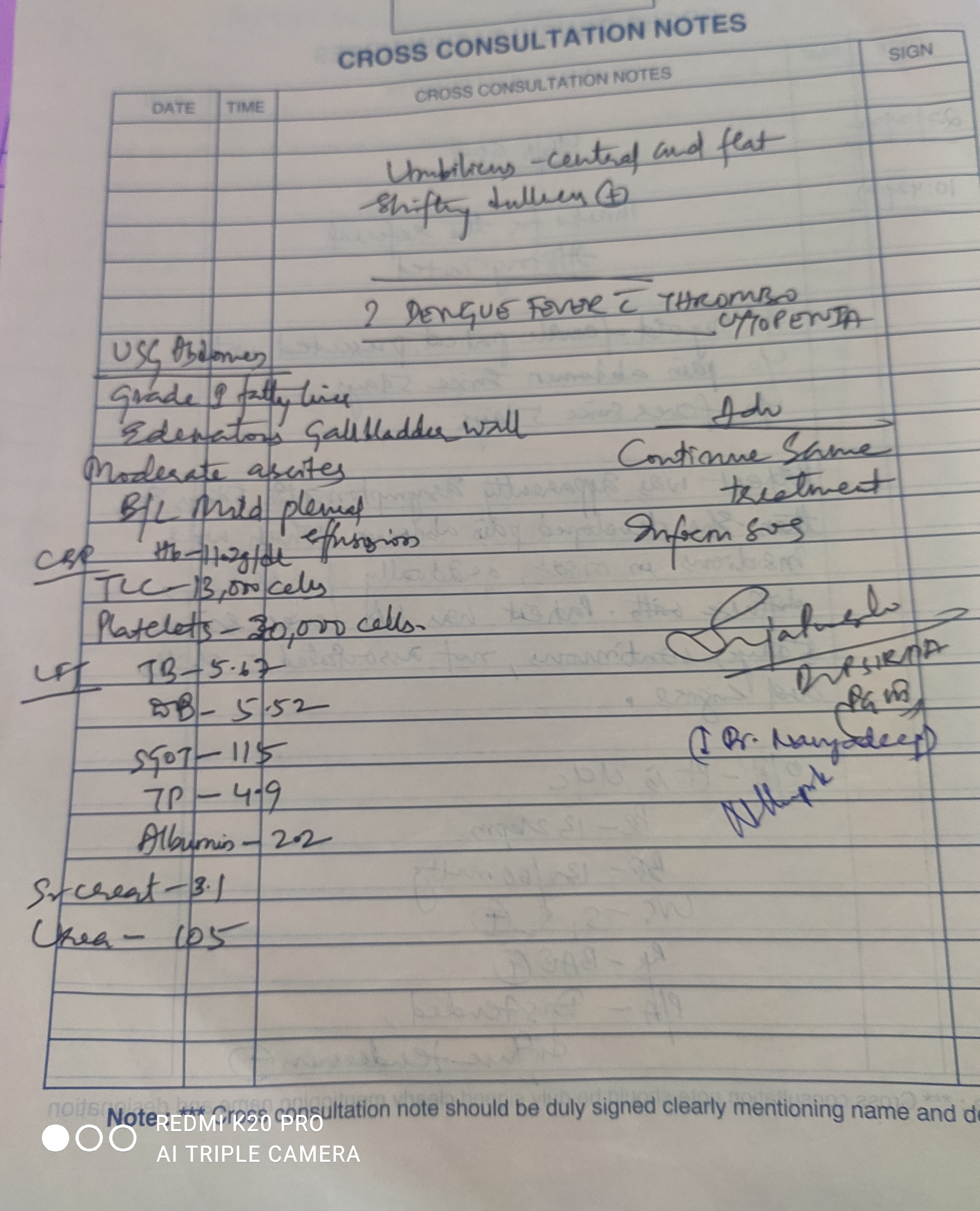
TB: 5.67. 6.25. 9.23 10.9. 8.34
DB:5.52. 6.15. 5.13 8.03. 6.37
AST:115. 485. 65 609. 1213
ALT:180. 189. 676 739. 531
ALP:500. 485. 547 392. 431
Total proteins:4.9. 4.9. 5.1 5.9. 6
Albumin:2.2. 2.6. 2.84 2.9. 2.94
RFT:
Day-1. Day-2. Day-3.
Blood urea: 105mg/dl. 124mg/dl 122mg/dl,118 mg,/dl (2pm) d-4 :
Serum creatinine: 3.1mg/dl. 3.5mg/dl. 3.6mg/dl ,2.7 m g/dl
Serum electrolytes:
Sodium:133. 124. 130. 137
Potassium:3.9. 3.5. 3.0. 3.0
Chloride:103. 101. 101. 104
Ionized calcium:0.86. 0.86. 0.85. 0.88
Phosphorus:5.6
Calcium: 9.8
Uric acid: 7.1
On1/1/23
S.urea:139
S,cr: 2.4
Electrolytes:
Na:140
K: 4.3
Cl:102
I ca:0.84
LFT:
TB:9.22
DB: 5.23
AST: 559
Alt: 390
ALP: 269
Tp:6.2
Alb: 3.07
A/G ratio: 0.98
2/1/23
.urea:139-128-55
S,cr: 2.4-1.9-1.2
Electrolytes:
K: 4.3-3.2-2.9-3.1
I ca:0.84-0.88
Ca 9.3-10
P; 3.9-2.8
Uric acid: 5.1-3.3
LFT:
TB:9.22-11.64- 16.06
DB: 5.23-10.14- 14.20
AST: 559-369-138
Alt: 390-346-126
ALP: 269-297-292
Tp:6.2-5.6-5.6
Alb: 3.07-2.9 -2.6
A/G ratio: 0.98-1.0-0.90
Urinary electrolytes:28/12/22
Na:133
K:11.7
Cl:198
Serum osmolality: 271 mosm/kg
Urine for ketone bodies : negative

Abg:
Ph:. 7.321. 7.408
Po2:. 101. 110
Pco2:. 16.4. 17.6
Hco3:. 12.4. 14.9
Na:. 127. 113
K:. 3.6. 3.5
Ca:. 0.57. 0.30
Cl:. 102. 88
Anion gap


29/12/22






USG abdomen:
Grade-1 fatty liver
Edematous gallbladder wall
Moderate ascites
B/l mild pleural effusion
Chest x ray:


Xray erect abdomen:


ECG:



2d echo
No RWMA
TrivialTr/Mr: no mr
Sclerotic Av, no As/ms
EF 60,RVSP:35mmhg
Good lv systolic function
No diastolic dysfunction, no pAH/PE
Icc size: 1.10 cms
Review 2d echo( 2/1/23)

Treatment:
Iv fluids @ 100ml/hr
Inj piptaz 2.25 gm/iv/Tid- d3
Inj vit k 1 ampoule in 100 ml NS iv/ od
Inj optineuron 1 ampoule in 100ml nd iv /od
T.doxy 100mg/RT/BD converted to oral on 1/1/23
Syp lactulose 30 ml RT/Hs converted to oral on1/1/23
RT feeds milk 100 ml 4th hrly stopped on 1/1/23
Fluids 50 ml hrly
Inj N acetyl cysteine (1ml=200mg)
100mg/hr(continuous iv infusion)
Zinc oxide cream for local application
Position change every 20 minutes
Daily bed sore dressing
3Hemodialysis sessions done
1sdp+ 2 FFP transfusions done out side
1 sdp+ 3ffp transfusions done
5 ffp transfusion done on 31/12/22

Comments
Post a Comment