74Male with aphasia and seizures
ICU bed 1 :
A 74 years old male patient,resident of kondaram ,gauraram mandal nalgonda district,married 50years ago,who is an agricultural labourer by occupation(plant paddy ,cotton )was referred from outside hospital,in view of lost of speech since 10 days.
He was apparantly assymptomatic 25 years ago,then he went to bombay to her sisters house who stays there,and on his return to his kondaram village,got fever for 1 week and relieved on medication and on routine investigations was diagnosed as having OHA since then,initially 1tablet per day and on futhur followup increased the dosage to 1——-X———1/2 tab,and was apparantly assymptomatic till 17 years ago and then developed pedal Edema till knees,yellowish discolouration of eyes and shortness of breath on exertion for which he got admitted in our hospital for 8 days and was managed conservatively,and was asymptomatic for 7 years and then 10years ago,he had history of fever ,low grade associated with evening rise of temperature and cough for 10 days and was diagnosed as ?sputum positive tuberculosis and was treated with ATT for 2 years(acc to his wife),and was assymptomatic 3 years back and then developed pain in the right loin for 10 days for which they went to local hospital and told as having a renal calculi and was kept on conservative management but the pain didn’t subsided even on using medication for 6 days and then ?stent /?foleys was placed ,but still his pain didn’t subsided associated with new onset fever,and then they removed the placed stent ,but still the pain at the right loin persisted a surgery was done?lithotripsy ,and then again went to other hospital as they were told that calculi wasn’t removed completely and again stent was placed >>it got infected and seen as pus filled mass at the right loin and then surgery was done and pain got relieved,and he was alright till 4 mnths and then he had a small abrasion /small crack over left second toe initially and then he got injured to the same finger by accidentally hitting it to wall,>>>swelling over that finger >>>blackish discoloured in 8days>>>amputated the second toe,and the skin of the adjacent toe was also removed,at the same time he had left hand dragging pain for which investigations were done and treated with muscle relaxants and PPIs and after 2 days due to imbalance over that amputated foot ,he had history of fall at 2:00am in the night when he went to washroom,and went lo hospital and was told as ?Intertrochantric fracture and ?hemiarthroplasty was done,and during the postoperative period patient used to have brief episodes of altered sensorium over a transient period,for which an MRI /CT was done and was told as having an extraaxial mass in the brain(?neoplasm),and the episodes of altered sensorium/hallucinations once/twice in a week(Eg:He mistakened the hanged clothes as persons,and used to talk with persons who expired)
And 2 months ago ,he developed pain in the right hypochondrium dragging type and got admitted in hospital and was treated conservatively for 10 days,and told as having ?cholelithiasis ,and 10 days ago in the afternoon he ate rice and at 3:00pm he had a pomegranate fruit and at 4:00pm he was sleeping on the bed and when his wife called her,he had no response on calling him(lost his speech),(eyes open )and she thought it as hypoglycaemic episode and poured sugar in his mouth but he was not having it,and at the same time he had involuntary rolling over the bed and stiffened mouth(unable to open) and had involuntary micturition at that time and rmp arrived and his Bp and grbs was normal and they took them to hospital and during travelling he had deviation of mouth to right,they(attenders)thought it as hemiparesis,and at hospital his SBP was 240mmHg,and on medication the deviation got corrected and on day 2 of admission due to decrease in saturation ,patient was intubated on 8-7-2023 and extubated on 14-07-2023.
Post extubation,no return of his speech and there were absent tongue moments also.
K/c/o Diabetes since 15 years,on OHA initially,shifted to insulin since 1 year.
K/c/o CKD since 4mnths and on conservative management
On regular checkup was diagnosed as having hypertension since 2 years and on regular medication.
Diet is mixed
Previously he used to have,gatka in mrng and rice in afternoon and night,but since 4mnths gatka in the mrng,rice afternoon,java at 3pm and at 8pm.
Decreased Apetite since 20 days.
Constipation since 15days
Chronic Alcohol intake for 30years stopped 3 years ago ,smoker for 20 years stopped 2 years ago.
At the time of presentation:
Pt is confused
GCS:E4V1M6
BP:150/70mmHg
PR:98bpm
RR:18cpm
RS:clear lungs
CNS:
Pt is obeying commands
Bilateral pupils normal in size and reacting to light.
Tone increased in bilateral upperlimbs
Normal in lowerlimbs
Power:couldn’t be elicited
But moving all 4 limbs to pain
Reflexes:
++ in both biceps,triceps and Supinator.
Bilateral lowerlimb reflexes absent.
Patient developed xerosis/dryskin over bilateral palms and legs and soles(since the past 10 days of his ICU admission)
Final diagnosis:
Aphasia (Global)secondary to mass in right frontal lobe
With acute kidney injury on CKD
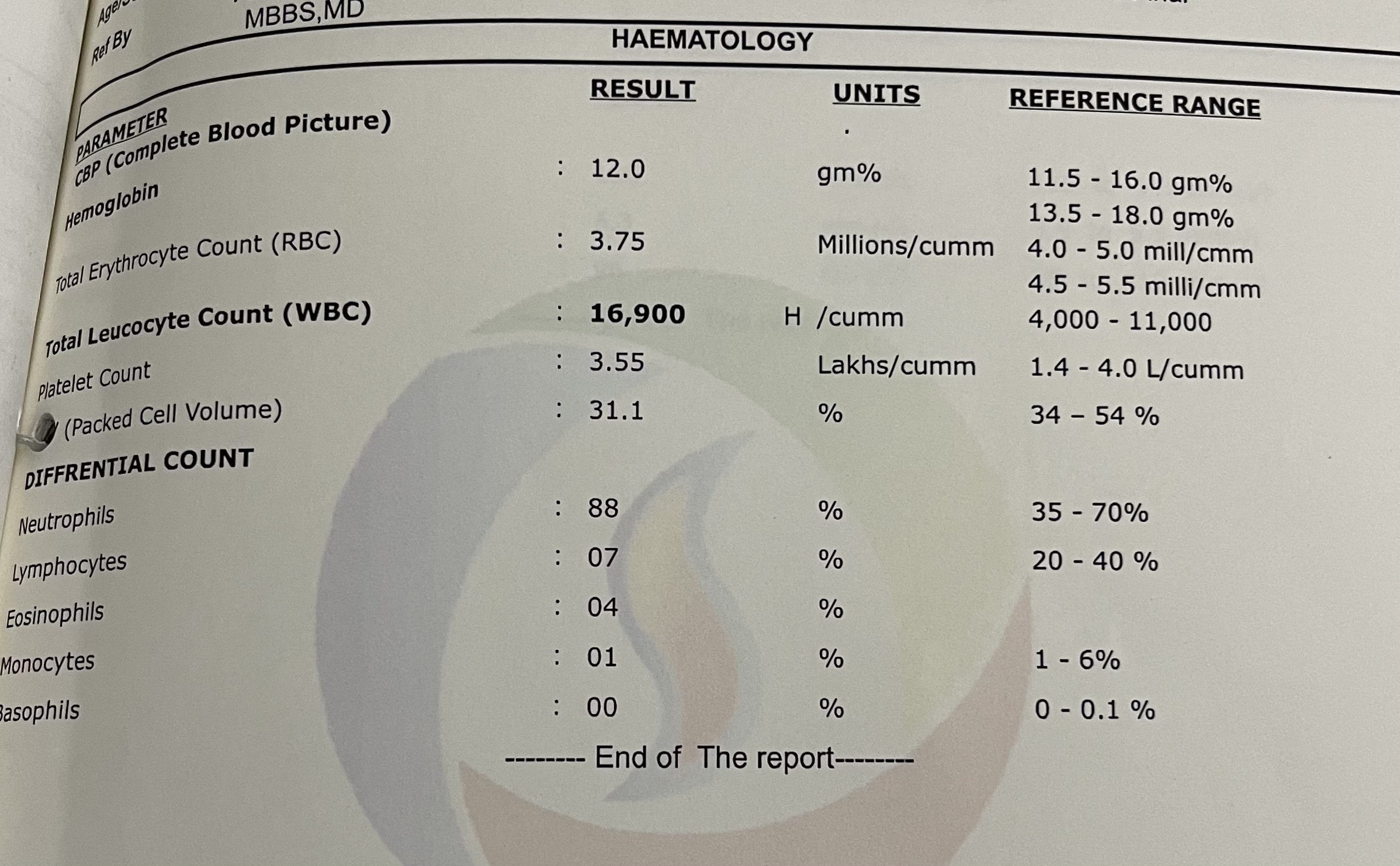
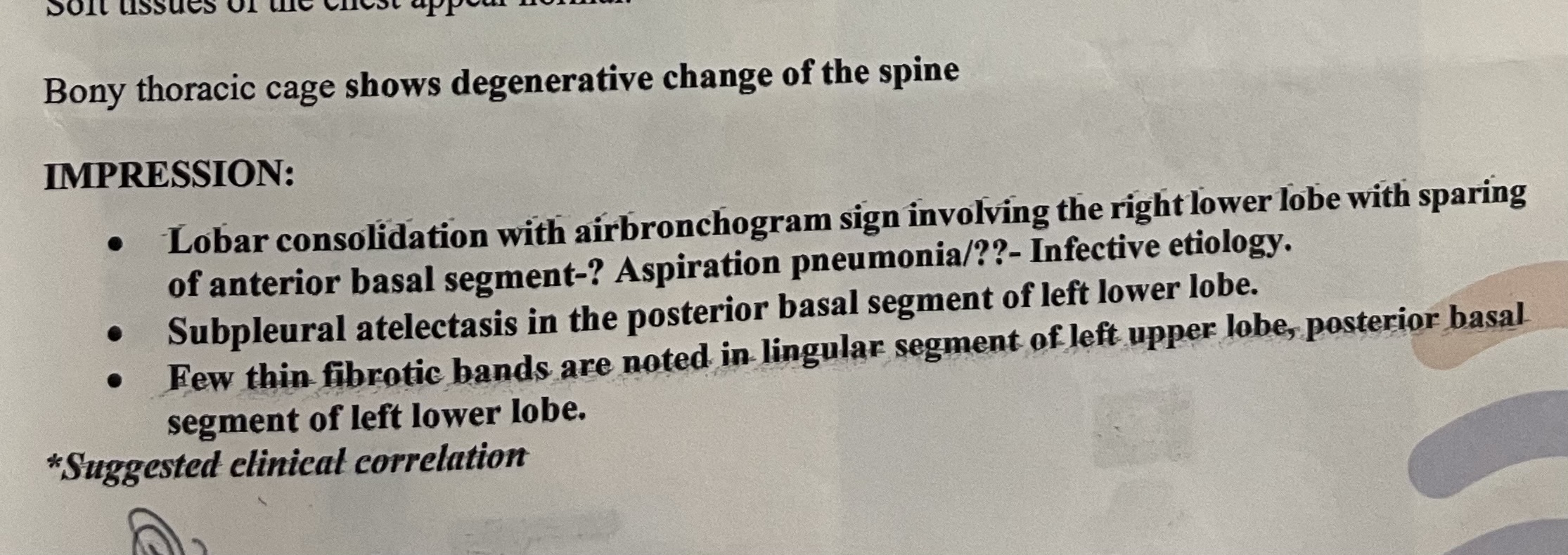
Investigations- (09/07/2023)







On 10/07/2023


USG- Abdomen

On 11/07/23



On 12/07/23



On 13/07/23




On 14/07/23



















Questions around this patient :
1)cause of his sudden aphasia,
2)If the mass in the frontal lobe is the cause,why would it cause sudden aphasia?
3)cause for his hypertonia of his upperlimbs
Starter Answers :
1) Compression of motor and sensory speech areas due to focal raised ICT caused by the focal lesion
2) Sudden rise of focal pressure such as bleed into the mass or infarct into the mass or if the mass was a living parasite, it's sudden death and consequent inflammation
3) Compression of the inhibitory interneurons in the UMN pyramidal fibers traversing the subcortical areas of the frontal lobe as well as brain stem
Plan:For Steriotactic biopsy
Coming to complexities sir:
They live in a house in kondaram,own house
The patient had one younger sister ,and his wife has two brothers and one sister.
The first insult was 50years ago,as they tried for children visited many hospitals but they didn’t have any children.
And they have no agricultural land for themselves, they have 2 buffaloes where they could earn some money by selling their milk,but he sold them 20 years ago,as he was diagnosed as diabetes(and found himself weak and that was when he stopped working)and due to financial issues.
And other insult was 3 years ago,when he lost his younger sister(died due to ?seizures?paralysis with uncontrolled diabetes),and some Arguements went on after her sister death,because they have many loan’s (as she died without clearing those)
And other insult was 3 years ago when they got their kidney operation for renal calculi,where they have spend 4lakh rupees
Other insult,when he got his finger amputation (spend Rs:53,000/-)
And for hemiarthroplasty for which they spend (Rs:40,000/-)
For cholilithiasis(Rs:42,000/-)
During all these period as the patient is consious and well oriented he used to say to his wife ,that his savings are getting over.
These are the insults faced by the patient uptill 6-07-2023.
And then now insult to his wife,as they spend 2lakh rupees in outside prvt hospital and acc to his wife,now they are getting money frm her brothers.
Comments
Post a Comment