CVA ?PCA STROKE ,WITH ACUTE INFARCT IN CEREBELLUM
This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input
. This E-blog also reflects my patient's centred online learning portfolio.
A 57 year old male who is a autodriver,by occupation came with complaints of
Giddiness since 4 days
Excessive sweating since 4days
Swaying towards right since 4 days.
HOPI: Patient was apparently asymptomatic 5 days ago,and then developed pain and swelling of bilateral lateral malleolus,for which he visited he visited local RMP,for which he received an injection?not known,followed by which ,he developed excessive sweating and giddiness and difficulty to walk ,associated with swaying to right ,for which he went to a local hospital and was advised to get a CT done,and medications were given,and referred here for further management,and while at admission he is consious,coherent and oriented ,and his blood pressure was 170/100mmhg,and giddiness is present.
Diplopia present, for a brief period of 30 minutes.
Horizontal nystagmus,fast beating towards right.
No dysphagia,ptosis,miosis and anhydrosis
No history of hiccups
No history of headache,nausea,vomiting
No history of blurred vision
No deviation of mouth and drooling of saliva
No involuntary moments.
Past history: No similar complaints in the past
Personal history:Mixed diet
Apetite Normal
Sleep adequate
Bowel and Bladder moments regular.
Addictions: Chronic alcoholic since 20 years, stopped 2 years back
Chronic beedi smoker since 22 years.
Family history:No significant family history
GENERAL EXAMINATION:
Patient is moderately built and nourished.








Bp:160/80mmHg in left arm in sitting position
PR:86bpm
RR:16Cpm
BAE present.NVBS Present
CVS:S1S2 heard
CNS:
HIGHER MENTAL FUNCTIONS:
Oriented to time place and person
Immediate memory:Intact
Short term memory:Intact
Longterm memory:Intact
No delusions and hallucinations.
CRANIAL NERVES:
Olfactory nerve(I): Smell is intact
Optic nerve(II):size of both pupils equal.
Pupil reactivity to light:present
Direct and indirect light reflex are present in both eyes.
Oculomotor(III),Trochlear(IV)and Abducens(VI):ocular movements present.Brief period of diplopia,No ptosis,Horizontal Nystagmus Present
Trigeminal(V): Sensations over the face present.
Corneal reflex:present
Jaw jerk: Absent.
Muscles of mastication:Normal(No wasting)
Facial nerve(VII): No deviation of mouth
The wrinkles on both sides of forehead are present.
Taste:intact.
Secretions:Normal in eyes.
Vestibulocochlear nerve(VIII):Hearing intact.
No positional vertigo and nystagmus.
Glossipharyngeal (IX) and Vagus(X): uvula is centre and pilatoglossus pillars are normal and gag reflex intact.
Taste sensations from posterior tongue is normal.
Spinal accesory(XI):Trapezius and Sternocleidomastoid normal.
Hypoglossal(XII): Tongue (opening )central in postion.
No weakness and wasting of tongue.
Tongue moments normal.
MOTOR SYSTEM:
No visible muscle wasting is seen on inspection.
TONE OF THE MUSCLE:
Right: upper limb—Normal tone
lower limb—Normal tone
Left:Upper limb—-Normal tone
lower limb—-Norma tone.
POWER OF MUSCLE:
Right upper limb: 5/5
(Tested for supraspinatus,Deltoid,infraspinatus,Rhomboid,pectoralis major,latissimus dorsi,biceps, brachioradialus, triceps,Extensor carpi radialis, Extensor carpi ulnaris,Extensor digitorum,Flexor carpi radialis and Flexor carpi ulnaris,Abductor pollicis longus, Extensor pollicis brevis,Extensor pollicis longus,Lumbricals,Abductor digiti minimi.)
Right lower limb:5/5
(Tested for Quadriceps femoris,Tibialis anterior,Tibialis posterior,Gastrocnemius,peronei,Extensor digitorum longus,flexor digitorum longus,extensor digitorum brevis,extensor hallucis longus)
Left upper limb:5/5
Left lower limb:5/5
POSTURE AND GAIT:
Broad based gait
No involuntary movements or tremors are seen.
SENSORY SYSTEM:
Fine touch, crude touch and pain intact in all four limbs.
Temperature: Differentiation of cold and hot objects is seen.
Joint postion:5/10 (incorrect)in Right lowerlimb and 5/10 (incorrect)in left lower limb.
No abnormal sensations are present.
REFLEXES:
Tendon reflexes:
Jaw jerk: Not seen
Right:
Biceps jerk:+++
Triceps jerk:+++
Supinator jerk:+++
Knee jerk:+++
Ankle jerk:+++
Left side:
Biceps jerk:+++
Supinator jerk:+++
Triceps jerk:+++
Knee jerk:+++
Ankle jerk:+++
Superficial reflex:
Abdominal reflex: present
Plantar reflex: of right side: Plantarflexion
Left side: mute
Cerebellar function tests:
Titubation absent
Trunkal ataxia/gait ataxia swaying towards right
No dysarthria,tremors,hypotonia
Coordination tests:
Finger nose test: done by both hands(normal).
No overshooting.
Finger to finger testing:no incordination.
Diadokokinesia: normal with right hand.
Heel knee test: no incordination
Rhombergs test: swaying towards right with eyes open
CVA ?PCA stroke
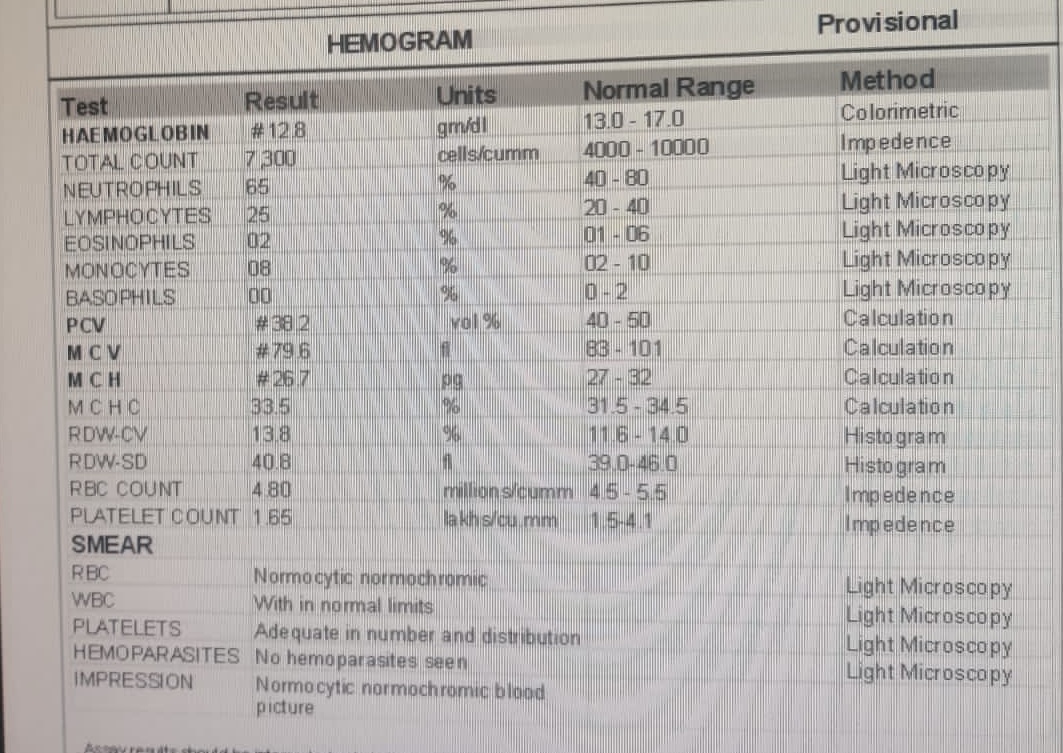
INVESTIGATIONS:







FINAL DIAGNOSIS:

Comments
Post a Comment